GENERAL PHYSICAL EXAMINATION:
patient is conscious, coherent,cooperative and moderately built and moderately nourished
VITALS:
→ patient is afebrile
→ BP-110/80 mm Hg
→ PR-70 bpm
→ RR-16 Cpm
✓SpO2- 98%
✓GRBS - 122gm/dl
No Pallor, Icterus, Cyanosis, clubbing, Odema, lymphadenopathy.
ON INSPECTION:
red erythematous lesions Over Hands, legs, Palms and Soles including Web Spaces
{kind=link}



CNS EXAMINATION:
- Higher mental functions-normal
- Cranial nerves- intact
- Sensory system- normal
- Motor system- normal
- Meningeal signs- absent
- Cerebellar signs- absent
CVS EXAMINATION:
INSPECTION:
No scars sinuses and engorged ve
No visible pulsation
PALPATION:
apical impulse : heard in fifth inter coastal spac
ASCULTATION:
S1 and S2 heard
No murmurs
RESPIRATORY SYSTEM EXAMINATION:
INSPECTION OF UPPER RESPIRATORY SYSTEM:
oral cavity- normal
Nose- normal
Pharynx- normal
LOWER RESPIRATORY TRACT:
INSPECTION:
trachea: central
Symmetry of chest : symmetrical
Movement: B/L symmetrical expansion of chest respiration
No scars, engorged veins or sinuses.
PALPATION:
All inspectory findings are confirmed by palpation.
Trachea: central - confirmed by three finger test.
Assessment of anterior and posterior chest expansion- B/L symmetrical expansion of chest.
No chest wall tenderness
Vocal fremitus- normal
PERCUSSION:
done in sitting position
Resonant
AUSCULTATION:
Vesicular breath sounds heard
Bilateral air entry present
No added sounds
ABDOMINAL EXAMINATION:
INSPECTION:
Shape : elliptical
Quadrants of abdomen moving in accordance with respiration.
Umbilicus- central and inverted
No scars sinuses or engorged veins
PALPATION:
No tenderness
No organomegaly
PERCUSSION:
tympanic
ASCULTATION:
Normal
No organomegaly , no tenderness.
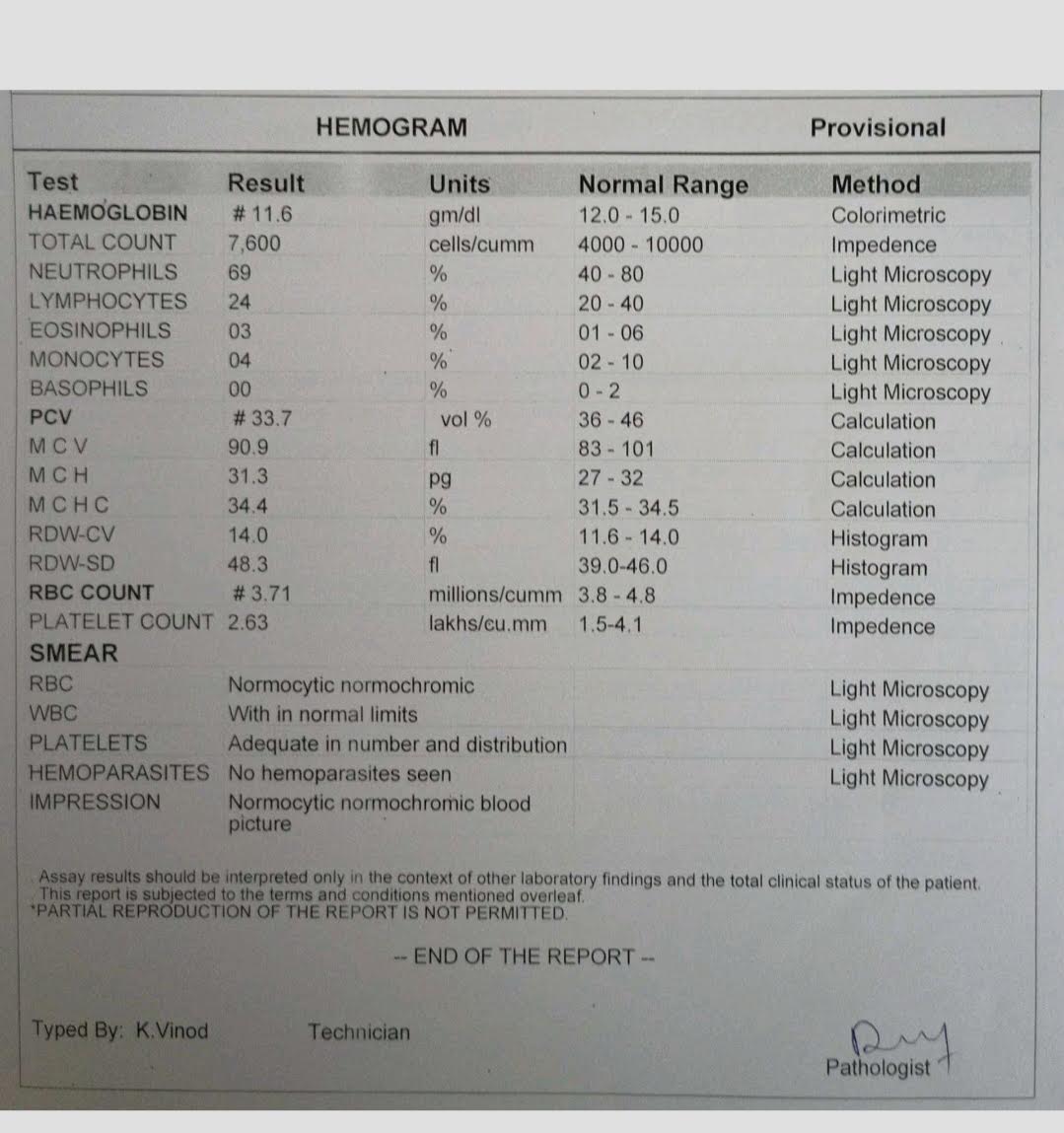
INVESTIGATION REPORTS:



{kind=link}




{kind=link}
PROVISIONAL DIAGNOSIS: - HENOCH SCHONLEIN PURPURA ( Leucocytoclastic Vasculitis)
TREATMENT:
At present patient is using:
Tab. Dapsone 100mgS
Syruporofer 5mlT
Tab Shelcal






Comments
Post a Comment